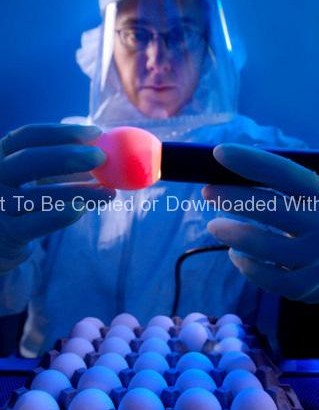
This 2005 photograph of the Centers for Disease Control and Prevention’s Dr. Terrence Tumpey, one of the organization’s staff microbiologists and a member of the National Center for Infectious Diseases (NCID), showed him examining reconstructed 1918 Pandemic Influenza Virus inside a specimen vial containing an orange-colored supernatant culture medium.
Dr. Tumpey, here seen in a Biosafety Level 3-enhanced laboratory setting, was working beneath a flow hood, which pulls air from outside the hood into the hood’s confines, and is then filtered of any pathogens before being re-circulated inside the self contained laboratory atmosphere.
Dr. Tumpey recreated the 1918 influenza virus in order to identify the characteristics that made this organism such a deadly pathogen. Research efforts such as this, enables researchers to develop new vaccines and treatments for future pandemic influenza viruses.
The 1918 Spanish flu epidemic was caused by an influenza A (H1N1) virus, killing more than 500,000 people in the United States, and up to 50 million worldwide. The possible source was a newly emerged virus from a swine or an avian host of a mutated H1N1 virus. Many people died within the first few days after infection, and others died of complications later. Nearly half of those who died were young, healthy adults. Influenza A (H1N1) viruses still circulate today after being introduced again into the human population in the 1970s.